The pumping mechanism of the heart is adjusted by the network of coronary arteries and cardiac veins . Myocardial infarction ocurs when the blood supply is disrupted . In the progressive form , this may lead to heart failure .
The repopulation of the scar is achieved through various methods . One of them is to use autologous bone marrow cells . Another strategy is to differentiate the cardiac progenitor cells ( CPC ) . A third direction is to use cardiomyocytes ( CMs ) derived from human embryonic stem cells ( hESC ) , hESCs cardiac progenitor cells ( hESC - CPC ) , human pluripotent stem cells ( hPSCs ) , or human induced pluripotent stem cells ( hiPSCs ) for the transplantation in the myocardium .
The review paper Concise review : reprogramming strategies for cardiovascular regenerative medicine : from induced pluripotent stem cells to direct reprogramming analyses more than a hundred papers . Three reprogramming strategies for the myocardial regeneration are brought in discussion ( figure 1 ) : the iPSCs technology , the partially reprogramming method and the direct set of approaches .
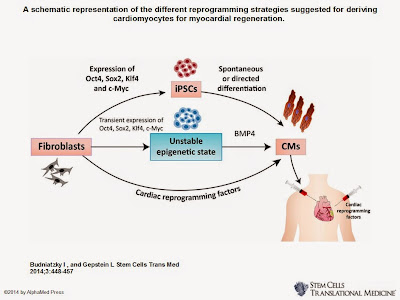
Figure 1 . The CMs derived from the iPSC ( top ) , the partial reprogramming ( middle ) , and the direct reprogramming technology ( below ) .
The hESCs represent the first reliable source for cardiomyocytes in vitro . The immune rejection , and the patient – or disease – specific hESCs are two challenges for the clinical allogeneic cell transplantation .
The hESCs and hiPSCs may generate beating cardiomyocytes in an inefficient method . The canonical Wnt pathway uses hiPSCs and small molecules in a more efficient signaling strategy .
Cardiomyocytes are partially reprogrammed from the iPSCs through a technology developed in 2006 . It takes a few months to differentiate the colonies of hiPSCs into the cardiac lineage . The use of partially reprogrammed cells reduces the length of time for the process to 11 – 12 days . There are also challenges for reaching the clinical practice ( figure 2 ) . Some of them are : the phenotypic heterogeneity of the differentiating CMs , the tumorigenic risk , and the poor in – vivo survival .

Figure 2 . The phases and challenges of the partially reprogrammed iPSCs method towards clinical practice .
The process of direct reprogramming of fibroblasts into induced cardiomyocyte cells ( iCMs ) is epigenetically stable . It is achieved through various combinations : by adding the Hand2 to the Gata4 , Mef2c and Tbx5 combination of transcription factors ; by using myocardin , and a combination of the Mef2c and Tbx5 transcription factors ; through a combination of a Janus inhibitor and four microRNAs ; by mixing two microRNAs and four transcription factors . The challenges of the myocardial regeneration are reduced through the deliver of reprogramming factors directly to the cardiac tissue .
Progress in the regeneration therapy is achieved if further studies are performed on early stages of myocardial infarction , if the stem cells delivered in – vivo generate efficiently new myocardium , and if the newly developed myocardium has suitable performance for the patient .